St. Jude unveils powerful resource to advance treatment of pediatric solid tumors
St. Jude Children’s Research Hospital is offering the global scientific community no-cost access to an unprecedented collection of pediatric solid tumor samples and data to fuel research and move treatment forward
(MEMPHIS, Tenn. – Aug. 30, 2017) In an effort to improve outcomes for patients with some of the deadliest childhood cancers, St. Jude Children’s Research Hospital scientists have created the world’s largest collection of pediatric solid tumor samples, drug-sensitivity data and related information and have made the resource available at no charge to the global scientific community.
St. Jude and the Howard Hughes Medical Institute collaborated to create the resource, known as the Childhood Solid Tumor Network. The work is reported today as an advance online publication in the scientific journal Nature.
“Survival rates for children with recurrent solid tumors have not improved significantly in more than 20 years and remain below 30 percent,” said corresponding author Michael Dyer, Ph.D., chair of the St. Jude Department of Developmental Neurobiology and a Howard Hughes Medical Institute investigator. “This research will change that by promoting scientific collaboration to leverage the efforts of researchers worldwide to advance understanding and ultimately treatment of pediatric solid tumors.”





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
.@StJudeResearch unveils powerful resource to advance treatment of pediatric solid tumors Tweet
The project has already helped identify children with the muscle tumor rhabdomyosarcoma as the pediatric solid tumor patients most likely to benefit from combination chemotherapy that includes the experimental drug AZD1775. Planning has begun to incorporate the finding into an ongoing national clinical trial of the combination therapy for certain high-risk pediatric solid tumor patients.
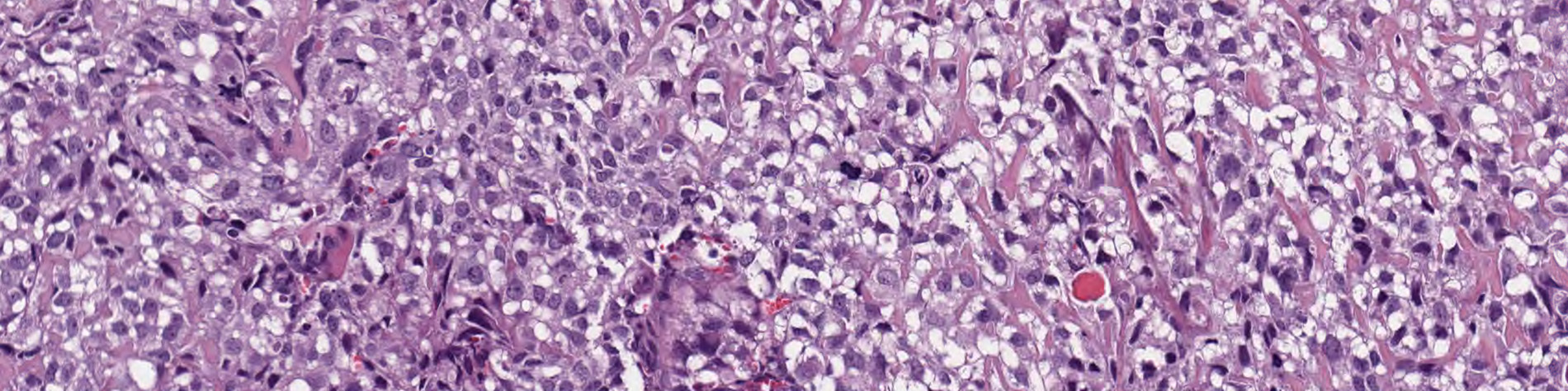
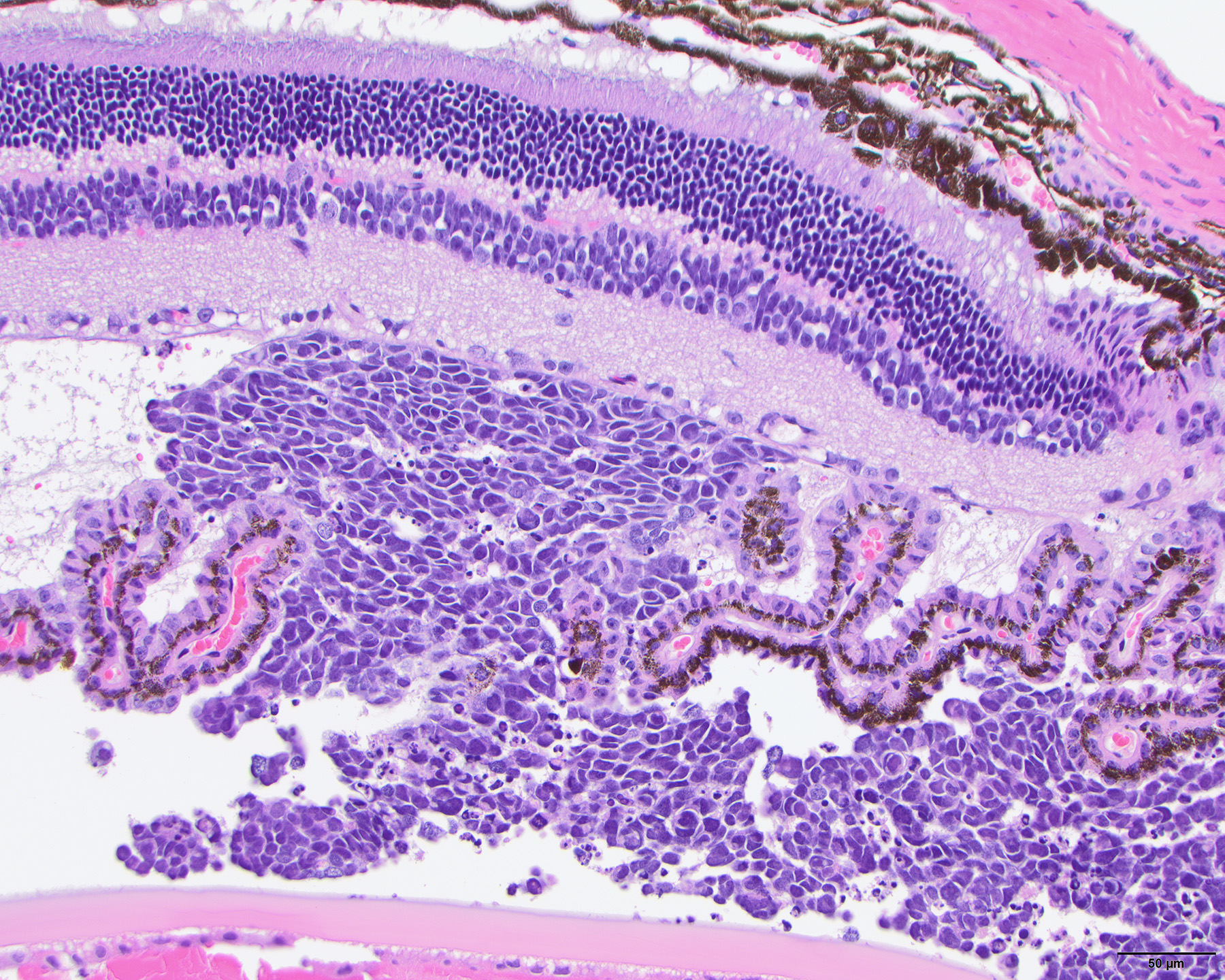
Pediatric solid tumors are rare and so are the tissue samples and other resources needed to advance their understanding and treatment. Solid tumors of the bone, muscle, kidney, eye and other organs excluding the brain account for about 30 percent of childhood cancers. While the overall cure rate for these pediatric solid tumors is 75 percent, long-term survival is much lower for the approximately 30 percent of patients whose tumors return.
The Childhood Solid Tumor Network was created to share the patient tumor samples and other scientific resources Dyer and his colleagues have developed by learning to grow human tumors in the same organ in mice. The network now includes samples from more than 67 different patient tumors representing 12 types of pediatric solid tumors. Along with the tumor samples, information about the drug sensitivity, pharmacokinetics and the molecular make-up of the tumors is also available. Accessing the data requires no commitment to collaborate with St. Jude scientists.
The network has significantly expanded scientific resources for pediatric solid tumor research. For example, through the Childhood Solid Tumor Network, investigators studying the bone cancer osteosarcoma have an additional 20 patient tumor samples available for research to supplement five osteosarcoma cell lines now widely used to study the tumor. For the eye tumor retinoblastoma, available resources increased from two cell lines that have been widely used for research to an additional 18 retinoblastoma tumor samples.
“When the St. Jude–Washington University Pediatric Cancer Genome Project started to sequence the complete tumor and normal genome of pediatric cancer patients, we realized we needed better models to take full advantage of the discoveries,” Dyer said. The genome project, which began in 2010, sequenced the genomes of more than 800 children and adolescents with some of the least understood and most difficult to treat cancers.
With the consent of patients and parents, researchers developed a system to grow St. Jude patient tumors in the same organ in mice. Such tumors are called orthotopic patient-derived xenografts. The standard approach has been to grow patient tumors in the flank of mice.
“The tumor samples were collected at diagnosis, recurrence and autopsy. Many came from patients with recurrent disease, which is important since previously we have had few models of recurrent pediatric solid tumors,” Dyer said.
In the first five years, tumor samples from the biopsies and surgical specimens of 168 St. Jude patients resulted in 67 pediatric solid tumors, representing neuroblastoma, osteosarcoma, Wilms tumor, retinoblastoma, rhabdomyosarcoma and other less common tumors. Patient identification was removed.
A comprehensive analysis comparing the original patient tumor to the orthotopic xenografts showed many orthotopic patient-derived xenografts retained their “molecular fingerprint” even after being grown in successive generations of mice. That suggests the tumors maintain their molecular identity when grown in the same microenvironment in mice and provide more accurate models for tracking tumor development and drug sensitivity, Dyer said.
Along with whole-genome and whole-exome sequencing and gene-expression profiling, the analysis included the most detailed examination yet of the genomic or clonal complexity of pediatric solid tumor orthotopic xenografts. Solid tumors include subsets of cancer cells called clones that have different mutations. Understanding and addressing clonal diversity is key to obtaining better cure rates because failure to kill all the clones in a tumor leaves the door open for cells from one clone to multiply and trigger a fatal relapse.
Researchers also demonstrated the potential of orthotopic xenografts to speed drug discovery and advance multi-drug chemotherapy. The scientists developed a new method that uses orthotopic xenografts to enhance sensitivity of drug screening to help identify the most promising compounds to move into clinical trials. The results, which include more than 500,000 data points on drug sensitivity, metabolism and related information, are available to the global biomedical research community in what is believed to be the world’s only free searchable database for childhood cancer.
Drug sensitivity screening helped researchers identify rhabdomyosarcoma as particularly sensitive to AZD1775, an inhibitor of the enzyme WEE1 that is involved in cell division and expressed at high levels in a variety of solid tumors. Investigators used orthotopic xenografts of high-risk rhabdomyosarcoma to show that the tumors responded when AZD1775 was combined with the chemotherapy drugs irinotecan and vincristine, which are currently used against rhabdomyosarcoma.
“This study shows that orthotopic patient-derived xenografts can serve as a bridge connecting basic and translational research to improve outcomes for patients,” Dyer said. “It serves as the gold standard for development, characterization and use of patient-derived tumors.”
Efforts continue to develop additional orthotopic patient-derived xenografts. The Childhood Solid Tumor Network now includes almost 100 pediatric solid tumors. Scientists plan to expand the effort to include induced pluripotent stem cells from children who are genetically predisposed to develop cancer. These are cells that have been reprogrammed to function as stem cells, which have the potential to become any cell type in the body.
The first authors are Elizabeth Stewart, M.D., and Sara Federico, M.D., both of the St. Jude Department of Oncology, and Xiang Chen, Ph.D., of the St. Jude Department of Computational Biology. The other authors are Anang Shelat, Cori Bradley, Brittney Gordon, Asa Karlstrom, Nathaniel Twarog, Michael Clay, Armita Bahrami, Burgess Freeman III, Beisi Xu, Xin Zhou, Jianrong Wu, Victoria Honnell, Monica Ocarz, Kaley Blankenship, Jason Dapper, James R. Downing, Jinghui Zhang, John Easton and Alberto Pappo, all of St. Jude; and Elaine Mardis and Richard Wilson of The Genome Institute, Washington University School of Medicine, St. Louis.
The research was funded in part by grants (CA21765, EY014867, EY018599, CA168875) from the National Institutes of Health, Alex’s Lemonade Stand Foundation for Childhood Cancer, the Tully Family Foundation, the Peterson Foundation, St. Baldrick’s Foundation, the National Pediatric Cancer Foundation, the Howard Hughes Medical Institute and ALSAC, the fundraising and awareness organization of St. Jude.
St. Jude Media Relations Contacts
Erin Seidler
Desk: (901) 595-0445
Cell: (515) 537-4465
[email protected]
[email protected]
Michael Sheffield
Desk: (901) 595-0221
Cell: (901) 379-6072
[email protected]
[email protected]
St. Jude Children’s Research Hospital
St. Jude Children’s Research Hospital is leading the way the world understands, treats and cures childhood cancer and other life-threatening diseases. It is the only National Cancer Institute-designated Comprehensive Cancer Center devoted solely to children. St. Jude is ranked the No. 1 pediatric cancer hospital by U.S. News & World Report. Treatments developed at St. Jude have helped push the overall childhood cancer survival rate from 20 percent to 80 percent since the hospital opened more than 50 years ago. St. Jude freely shares the breakthroughs it makes, and every child saved at St. Jude means doctors and scientists worldwide can use that knowledge to save thousands more children. Families never receive a bill from St. Jude for treatment, travel, housing and food — because all a family should worry about is helping their child live. To learn more, visit stjude.org or follow St. Jude on social media at @stjuderesearch.