FOR MEDICAL MEDIA ONLY
Ryzodeg® provides successful glycaemic control with fewer injections than a basal-bolus regimen
Vienna, Austria, Thursday 18 September, 2014/PR Newswire/ - Data presented today at the 50th Annual Meeting of the European Association for the Study of Diabetes (EASD) show that Ryzodeg® (insulin degludec/insulin aspart) administered twice daily, provides successful glycaemic control with fewer injections than a basal-bolus regimen1*.
Ryzodeg® is a combination of two distinct insulin analogues (insulin degludec and insulin aspart in the ratio of 70% and 30%), making it the first combination of a basal insulin with an ultra-long duration of action and a well-established mealtime insulin in one pen for people with type 2 diabetes2-4.
"Patients currently using basal-bolus regimens may need to take up to four daily injections, which can be a great burden and very inconvenient. Ryzodeg® is a new treatment option which provides proven glycaemic control, with fewer injections and reduced rates of hypoglycaemia compared to basal-bolus regimens," said Dr Helena Rodbard, the study’s principal investigator and endocrinologist in Rockville, MD, USA. "This new treatment offers the potential for a simple alternative to basal-bolus for patients who require intensification of basal insulin regimens," she added.
The study presented at EASD was a 26-week randomised multinational phase 3b trial, where patients previously treated with basal insulin were randomised to a regimen of either twice daily Ryzodeg®, or a basal-bolus regimen of once-daily insulin degludec plus two to four injections of insulin aspart1. The study did not meet its primary endpoint of non-inferiority; however, the results showed that HbA1c was reduced for patients on either regimen, to 7.0% and 6.8% respectively, with no significant difference between the two regimens1. Patients who received Ryzodeg® experienced a numerically lower rate of overall and nocturnal confirmed hypoglycaemic episodes1, 19% and 20% less, respectively. They also gained significantly less weight (p<0.05) over the course of the study and used a significantly lower daily insulin dose1 (12%; p<0.05) versus the basal-bolus regimen.
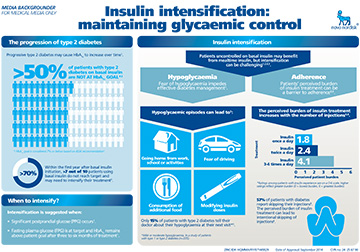
Type 2 diabetes is a progressive disease5, which means some patients will need to intensify insulin treatment eventually by adding mealtime insulin – bolus therapy – to achieve or maintain their glycaemic targets over time5. Studies have shown that more than 50% of people with type 2 diabetes on basal insulin alone are not achieving their glycaemic targets as measured by HbA1c6-8. Complications from diabetes caused by failing to keep optimal glycaemic control can be serious and may include problems such as heart disease, stroke, blindness, kidney disease, nerve damage and premature mortality9,10.
About Ryzodeg®
Ryzodeg® is a combination of two distinct insulin analogues, insulin degludec and insulin aspart in the ratio of 70% and 30%. In a multinational trial, Ryzodeg® delivered twice daily at main meals offered a successful reduction in HbA1c2,4 with lower risk of hypoglycaemia versus biphasic insulin aspart 30 in people with type 2 diabetes4. In other studies no apparent differences were shown between Ryzodeg® and its comparators, with respect to adverse events and standard safety parameters4,11-13. Ryzodeg® has been approved in Aruba, Brazil, Chile, Costa Rica, El Salvador, the EU, Hong Kong, Iceland, India, Israel, Japan, Kazakhstan, Macedonia, Mexico, Norway, Russia, South Korea and Switzerland.
About the clinical trial programme
The clinical trial programmes for insulin degludec (BEGIN®) and Ryzodeg® (BOOST®) comprise the largest in the field of insulin therapy, with more than 11,000 people included. Novo Nordisk completed the phase 3a BOOST® programme in 2010. This programme consisted of six randomised, controlled, treat-to-target trials in more than 30 countries. More than 2,000 people were included in the development programme. The programme was designed after consultancy with regulatory agencies in Europe, Japan and USA.
About Novo Nordisk
Headquartered in Denmark, Novo Nordisk is a global healthcare company with more than 90 years of innovation and leadership in diabetes care. The company also has leading positions within haemophilia care, growth hormone therapy and hormone replacement therapy. Novo Nordisk employs approximately 40,700 employees in 75 countries, and markets its products in more than 180 countries. For more information, visit novonordisk.com.
Further information
Media:
| Katrine Sperling | +45 4442 6718 | [email protected] |
|---|
Investors:
| Kasper Roseeuw Poulsen | +45 3079 4303 | [email protected] |
|---|---|---|
| Jannick Lindegaard Denholt | +45 3079 8519 | [email protected] |
| Daniel Bohsen | +45 3079 6376 | [email protected] |
| Frank Daniel Mersebach (US) | +1 609 235 8567 | [email protected] |
References
- Cooper JG, et al. Treatment intensification with IDegAsp BID vs IDeg OD plus IAsp in insulin-treated patients with type 2 diabetes: a randomised, controlled phase 3 trial. Oral presentation at the European Association for the Study of Diabetes (EASD) 50th Annual Meeting, Vienna, 15-19 September 2014.
- Ryzodeg® Summary of Product Characteristics (SPC). Bagsværd, Denmark, Novo Nordisk A/S; February 2014.
- De Rycke A, et al. Degludec – first of a new generation of insulins. European Endocrinology. 2011;7:84–7.
- Fulcher G, et al. Comparison of insulin degludec/insulin aspart and biphasic insulin aspart 30 in uncontrolled, insulin-treated type 2 diabetes: a phase 3a, randomized, treat-to-target trial. Diabetes Care. 2014;37:2084-90.
- Inzucchi SE, et al. Management of hyperglycemia in type 2 diabetes: a patient-centred approach: position statement of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2012;35:1364-79.
- Blak BT, et al. A retrospective database study of insulin initiation in patients with Type 2 diabetes in UK primary care. Diabet Med. 2012;29:e191-8.
- Dale J, et al. Insulin initiation in primary care for patients with type 2 diabetes: 3-year follow-up study.Prim Care Diabetes. 2010;4:85-9.
- Giugliano D, et al. Efficacy of insulin analogs in achieving the hemoglobin A1c target of <7% in type 2 diabetes: meta-analysis of randomized controlled trials. Diabetes Care. 2011;34:510–7.
- Imran SA, et al. Clinical practice guidelines: targets for glycaemic control. Can J Diabetes. 2013;37(Suppl.1):S31-4.
- Diabetes UK. Diabetes in the UK 2010: Key statistics on diabetes. Available at: http://www.diabetes.org.uk/Documents/Reports/Diabetes_in_the_UK_2010.pdf. Last accessed August 2014.
- Christiansen JS, et al. Superior FPG control and less nocturnal hypoglycaemia with IDegAsp vs BIAsp 30 in Asian subjects poorly controlled on basal or pre/self-mixed insulin: randomised phase 3 trial. Diabetologia. 2013;56(Suppl.1):S420 (abstract 1045).
- Hirsch IB, et al.Insulin degludec/insulin aspart administered once daily at any meal, with insulin aspart at other meals versus a standard basal-bolus regimen in patients with type 1 diabetes: a 26-week, phase 3, randomized, open-label, treat-to-target trial. Diabetes Care. 2012;35:2174-81.
- Onishi Y, et al. Superior glycaemic control with once-daily insulin degludec/insulin aspart versus insulin glargine in Japanese adults with type 2 diabetes inadequately controlled with oral drugs: a randomized, controlled phase 3 trial. Diabetes Obes Metab. 2013;15:826-32.
Novo Nordisk A/S
Corporate Communications
Novo Allé, 2880 Bagsværd, Denmark
Telephone: +45 4444 8888
Internet: www.novonordisk.com
CVR no: 24 25 67 90
ZINC ID: HQMMA/RY/0714/0030a
Date of approval: September 2014